Enterovesical fistula (Filling the urinary bladder)
- Native phase.
- Fill the bladder with minimum 100 mL NaCl + (1:10 contrast), e.g.:
- 10 mL contrast + 90 mL NaCl
- 20 mL contrast + 180 mL NaCl
- Repeat the native Phase.
- Venous phase (70-80s post-injection)
Rectovesical fistula (Rectal filling)
- Rectal filling with Gastrografin (30 mL + 1L NaCl). Infuse min. 500 mL
- Venous phase (70-80s post-injection)
Liver/Pancreas tumor
- Native Phase: liver
- CTA: thorax/liver
- Portal venous: liver
- Late venous: Complete abdomen
- Oral water: 500mL 10 min before exam, another 250 mL on CT-table
Anomalous pulmonary venous connection
- Venous phase over thorax
- Trigger in left atrium
- Flow: 3.5 – 4 max
- Contrast: 60 mL
Looking for aortic valve abscess
- ECG-gated coronary angiography + venouse phase over aortic valve (30s interscan Delay)
- Flow: 3 mL
- Contrast: 50 mL
Looking for Paraganglioma/Pheochromocytoma
- Neck + Thorax + Abdomen: arterial phase
- Abdomen: venous phase
Indications of oral contrast in abdominal CT
- Suspected perforation
- Postoperative anastomotic leakage
- GI-Fistula
- Oncologic staging
- Nonspecific acute abdomen
Postoperative oral contrast-protokols1
- Esophagus/gastric pullup: 100 mL of 5% gastrografin on the table
- Stomach/esophagojejunostomy/duodenum: 200 mL 5% gastrografin slowly, 5 min before scan
- Small bowel: 1000 mL 5% gastrografin slowly, 60 min before scan
- Rou-en-Y (gastrectomy + small bowel anastomosis): 300 mL 5% gastrografin slowly, 30 min before scan, 100 mL 5% gastrografin on table
Using water als contrast medium
- GI bleeding (two phases)
- Assessing mucosal enhancement of the bowel
- Assessing arterial supply of a pathologic process
Fasting before a CT exam
- 3 hours are enough
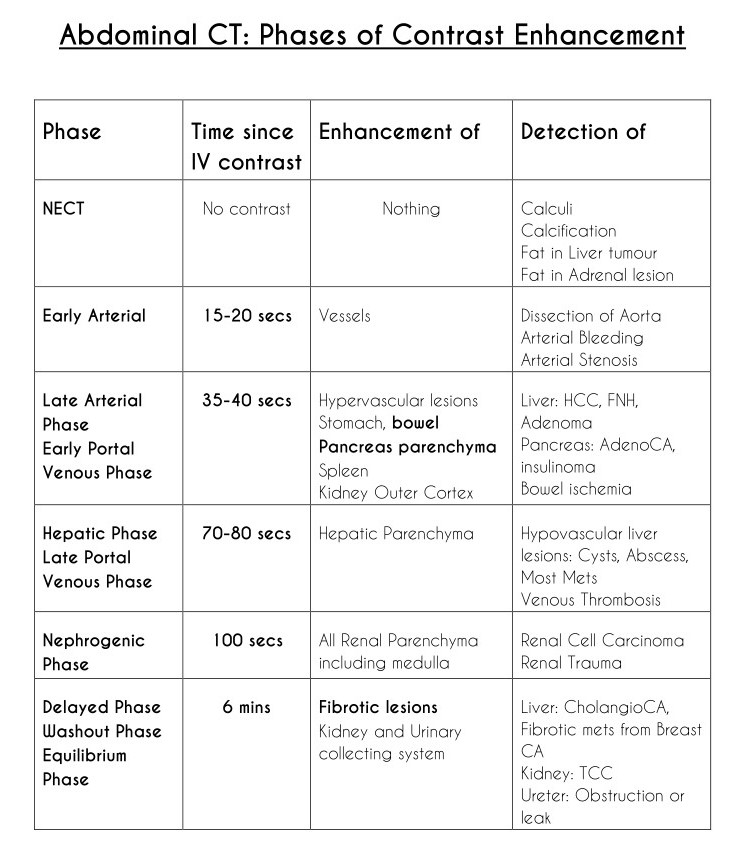
Abdominal CT: Phases of Contrast Enhancement
- RP 2020, Postop Abdomen – Vikas Shah[↩]